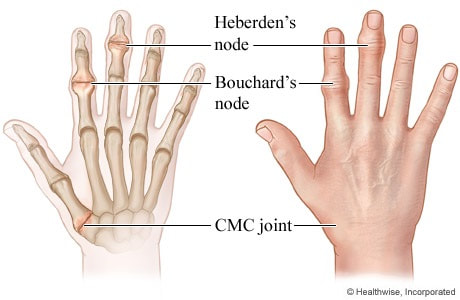
Heberden's and Bouchard's nodes in arthritis assessment (Rosen's 1510) are osteophytic spurs found on the hands.
Heberden’s nodes are caused by the formation of osteophytes due to repeated trauma at the joint and usually occurs during middle age. Mucous cyst: small, fluid-filled sacs that form between the DIP joint of the finger and the bottom of the fingernail.
Bouchard’s nodes are typically associated with limited motion of the affected joint.
Heberden’s nodes are caused by the formation of osteophytes due to repeated trauma at the joint and usually occurs during middle age. Mucous cyst: small, fluid-filled sacs that form between the DIP joint of the finger and the bottom of the fingernail.
Bouchard’s nodes are typically associated with limited motion of the affected joint.
Heberden's nodesDistal interphalangeal (DIP) joint (OA, not RA)
Heberden's nodes are higher up on the finger. Source: heberden's nodes disappear, dissolve heberden's nodes, reversing heberden's nodes, heberden's nodes natural treatment ... |
|
Bouchard's nodes |

|
|
|
Rheumatoid Arthritis (RA)
|
What is the Rheumatoid Factor (RF) blood test?
This is a blood test that measures rheumatoid factor, an antibody found in your blood. Your body produces antibodies when it detects harmful substances within your body. Four diseases in which an increase in RF are common are: Lupus, Sjogren's Syndrome, Scleroderma, and Rheumatoid Arthritis. A negative RF test does not completely rule out the disease; unless the test is faulty, it may be an indication this is your 'window of opportunity' to redirect the progression of the disease which requires dedication on your part. Western Medicine will address your symptoms; Alternative Medicine will address the cause. What is the Rheumatoid Factor (RF) blood test? An autoantibody is an antibody (a type of protein) produced by the immune system that is directed against one or more of the individual's own proteins. Many autoimmune diseases (notably lupus erythematosus) are caused by such autoantibodies. |
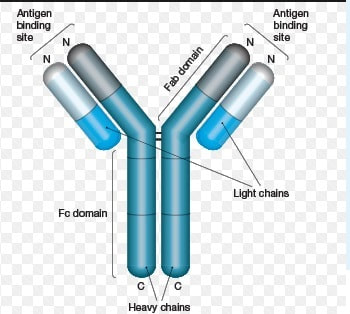
Antibodies, also referred to as immunoglobulins, are glycoproteins naturally produced in response to invading foreign particles (antigens) such as microorganisms and viruses. As such, they play a critical role in the immune system’s defense against infection and disease.
https://www.bio-rad-antibodies.com/immunoglobulin-antibody.html |
auto antibody – an antibody produced by the immune system that is directed against one or more of the individual proteins.
|
|
|
SURGERY
|
|
Longstanding rheumatoid arthritis commonly causes granulomalike rheumatoid nodules. PubMed search using “rheumatoid nodule in the brain” and 7 articles were found (1,2). A “rheumatoid endarteritis” search found 25 articles.
1. Karam NE, Roger L, Hankins LL, Reveille JD. Rheumatoid nodulosis of the meninges. J Rheumatol. 1994;21:1960–3.
2. Kim RC, Collins GH. The neuropathology of rheumatoid disease. Hum Pathol. 1981;12:5–15.
Rrapidly progressive dementia (1,2),
Heckman GA, Hawkins C, Morris A, Burrows LL, Bergeron C. Rapidly progressive dementia due to Mycobacterium neoaurum meningoencephalitis. Emerg Infect Dis. 2004;10:924–7.
Dr. Han argues that Mycobacterium neoaurum was “more likely a contaminant than the cause” and that the actual cause of death was most likely rheumatoid pachymeningitis. Dr. Han bases his argument on the absence of positive acid-fast stains or mycobacterial cultures and his assessments that the identification of M. neoaurum DNA was due to contamination and that the pathologic findings represented rheumatoid nodules.
Rheumatoid pachymeningitis is a rare complication of rheumatoid arthritis, in which patients may exhibit headache, cranial neuropathies, focal deficits, seizures, or cognitive dysfunction (5,6). Rheumatoid pachymeningitis usually, but not exclusively, occurs in patients with long-standing rheumatoid arthritis characterized by erosive disease and extra-articular manifestations, although the systemic disease may be quiescent when neurologic complications arise. Cerebrospinal fluid analysis is generally nonspecific. Magnetic resonance imaging may show prominent meningeal enhancement. Pathologic features may include vasculitis, rheumatoid nodules, and meningeal inflammation, with the latter 2 features being most common (5). The dura may demonstrate inflammation with fibrinoid necrosis (6). We reviewed the pathologic specimens of this case and confirmed the presence of abundant giant cells, endarteritis proliferans, and, most notably, extensive caseation necrosis typical of mycobacterial infection. We found no evidence of rheumatoid nodules, dural inflammation, or fibrinoid necrosis. Though this case does not satisfy Koch postulates, neither do most novel infectious diseases. Substantial international efforts were required to satisfy the postulates in the case of SARS (7). In this case, the identification of DNA from a “rare environmental mycobacterium” in a patient with overwhelming pathologic evidence of mycobacterial infection provides strong, though not foolproof, evidence of a possible causal role.
References
1. Han XY. Mycobacterium neoaurum contamination. Emerg Infect Dis. 2005;11: 1316–7.
2. Heckman GA, Hawkins C, Morris A, Burrows LL, Bergeron C. Rapidly progressive dementia due to Mycobacterium neoaurum meningoencephalitis. Emerg Infect Dis. 2004;10:924–7.
3. Chao SS, Loh KS, Tan KK, Chong SM. Tuberculous and nontuberculous cervical lymphadenitis: a clinical review. Otolaryngol Head Neck Surg. 2002; 126:176–9.
4. Ustianowski AP, Lockwood DNJ. Leprosy: current diagnostic and treatment approaches. Cur Opin Infect Dis. 2003;16:421–7.
5. Kato T, Hoshi K, Sekijima Y, Matsuda M, Hashimoto T, Otani M, et al. Rheumatoid meningitis: an autopsy report and review of the literature. Clin Rheumatol. 2003;22: 475–80.
6. Tan HJ, Raymond AA, Phadke PP, Rozman Z. Rheumatoid pachymeningitis. Singapore Med J. 2004;45:337–9.
7. Osterhaus ADME, Fouchier RAM, Kuiken T. The aetiology of SARS: Koch’s postulates fulfilled. Philos Trans R Soc Lond B Biol Sci. 2004;359:1081–2.
1. Karam NE, Roger L, Hankins LL, Reveille JD. Rheumatoid nodulosis of the meninges. J Rheumatol. 1994;21:1960–3.
2. Kim RC, Collins GH. The neuropathology of rheumatoid disease. Hum Pathol. 1981;12:5–15.
Rrapidly progressive dementia (1,2),
Heckman GA, Hawkins C, Morris A, Burrows LL, Bergeron C. Rapidly progressive dementia due to Mycobacterium neoaurum meningoencephalitis. Emerg Infect Dis. 2004;10:924–7.
Dr. Han argues that Mycobacterium neoaurum was “more likely a contaminant than the cause” and that the actual cause of death was most likely rheumatoid pachymeningitis. Dr. Han bases his argument on the absence of positive acid-fast stains or mycobacterial cultures and his assessments that the identification of M. neoaurum DNA was due to contamination and that the pathologic findings represented rheumatoid nodules.
Rheumatoid pachymeningitis is a rare complication of rheumatoid arthritis, in which patients may exhibit headache, cranial neuropathies, focal deficits, seizures, or cognitive dysfunction (5,6). Rheumatoid pachymeningitis usually, but not exclusively, occurs in patients with long-standing rheumatoid arthritis characterized by erosive disease and extra-articular manifestations, although the systemic disease may be quiescent when neurologic complications arise. Cerebrospinal fluid analysis is generally nonspecific. Magnetic resonance imaging may show prominent meningeal enhancement. Pathologic features may include vasculitis, rheumatoid nodules, and meningeal inflammation, with the latter 2 features being most common (5). The dura may demonstrate inflammation with fibrinoid necrosis (6). We reviewed the pathologic specimens of this case and confirmed the presence of abundant giant cells, endarteritis proliferans, and, most notably, extensive caseation necrosis typical of mycobacterial infection. We found no evidence of rheumatoid nodules, dural inflammation, or fibrinoid necrosis. Though this case does not satisfy Koch postulates, neither do most novel infectious diseases. Substantial international efforts were required to satisfy the postulates in the case of SARS (7). In this case, the identification of DNA from a “rare environmental mycobacterium” in a patient with overwhelming pathologic evidence of mycobacterial infection provides strong, though not foolproof, evidence of a possible causal role.
References
1. Han XY. Mycobacterium neoaurum contamination. Emerg Infect Dis. 2005;11: 1316–7.
2. Heckman GA, Hawkins C, Morris A, Burrows LL, Bergeron C. Rapidly progressive dementia due to Mycobacterium neoaurum meningoencephalitis. Emerg Infect Dis. 2004;10:924–7.
3. Chao SS, Loh KS, Tan KK, Chong SM. Tuberculous and nontuberculous cervical lymphadenitis: a clinical review. Otolaryngol Head Neck Surg. 2002; 126:176–9.
4. Ustianowski AP, Lockwood DNJ. Leprosy: current diagnostic and treatment approaches. Cur Opin Infect Dis. 2003;16:421–7.
5. Kato T, Hoshi K, Sekijima Y, Matsuda M, Hashimoto T, Otani M, et al. Rheumatoid meningitis: an autopsy report and review of the literature. Clin Rheumatol. 2003;22: 475–80.
6. Tan HJ, Raymond AA, Phadke PP, Rozman Z. Rheumatoid pachymeningitis. Singapore Med J. 2004;45:337–9.
7. Osterhaus ADME, Fouchier RAM, Kuiken T. The aetiology of SARS: Koch’s postulates fulfilled. Philos Trans R Soc Lond B Biol Sci. 2004;359:1081–2.
ENZYMES (http://cal.vet.upenn.edu/projects/saortho/chapter_86/86mast.htm)
Enzyme levels in synovial fluid have been studied extensively in humans and increases have been found to accompany various articular diseases. However, increases (or decreases) in specific enzymes that would allow a differentiation of one disease entity from another have not been demonstrable.
Enzymes are released into the synovial fluid from damaged tissue during phagocytosis and from the general circulation about the inflamed joint. Although their diagnostic significance is not great, the role enzymes play in destruction of articular tissue is important. Of particular importance are the collagenases, which specifically break down collagen of articular cartilage. Collagenases have been found in various inflammatory synovial fluids and especially in synovial fluid of animals with rheumatoid arthritis, where they are produced by the synovial membrane cells and by the polymorphonuclear leukocytes.(9) These enzymes probably account for the invasive properties of rheumatoid pannus.
Lactic dehydrogenase isoenzymes in synovial fluid have been studied in horses, and differences between normal and diseased joints have been found.(20) Apparently little work has been done to date on enzyme levels in canine and feline synovial fluid. Until such work is done, the presence of these substances in the synovial fluid of diseased joints in these animals can only be assumed.
PROSTAGLANDINS
Prostaglandins are a family of compounds comprising 20 carbon aliphatic unsaturated fatty acids.(26) Although first described in 1933, it is only recently that their physiological significance has begun to be appreciated. In relation to articular disease, it is now known that prostaglandin E, (PGE-1) plays a significant role in aiding or promoting the tissue destruction of rheumatoid arthritis.(25,26) Synovial fluid levels of prostaglandins in human rheumatoid arthritis patients are elevated far beyond those in normal joint fluid or joint fluid from patients with osteoarthritis. In vitro studies have shown increased prostaglandin synthesis by rheumatoid synovium and the promotion of bone resorption and articular cartilage destruction by prostaglandins.(27)
To date, data are not available describing prostaglandin levels in synovial fluid from a large number of normal dogs or cats or in those with disease. However, increased amounts of prostaglandins have been found in the joints of dogs injected with known inflammation producing substances, suggesting that, as in humans, synovium of the canine joint produces prostaglandins when inflamed.(10) Prostaglandin levels of synovial fluid have no great diagnostic significance as yet, but they may prove to be valuable in differentiating early immune-mediated synovitis from the synovitis of osteoarthritis.
sjogren
https://www.youtube.com/watch?v=C3e6V0tZIA4
https://www.youtube.com/watch?v=xN6tHrp1LVw&feature=emb_logo
https://www.sciencedirect.com/topics/medicine-and-dentistry/rheumatic-disease
Enzyme levels in synovial fluid have been studied extensively in humans and increases have been found to accompany various articular diseases. However, increases (or decreases) in specific enzymes that would allow a differentiation of one disease entity from another have not been demonstrable.
Enzymes are released into the synovial fluid from damaged tissue during phagocytosis and from the general circulation about the inflamed joint. Although their diagnostic significance is not great, the role enzymes play in destruction of articular tissue is important. Of particular importance are the collagenases, which specifically break down collagen of articular cartilage. Collagenases have been found in various inflammatory synovial fluids and especially in synovial fluid of animals with rheumatoid arthritis, where they are produced by the synovial membrane cells and by the polymorphonuclear leukocytes.(9) These enzymes probably account for the invasive properties of rheumatoid pannus.
Lactic dehydrogenase isoenzymes in synovial fluid have been studied in horses, and differences between normal and diseased joints have been found.(20) Apparently little work has been done to date on enzyme levels in canine and feline synovial fluid. Until such work is done, the presence of these substances in the synovial fluid of diseased joints in these animals can only be assumed.
PROSTAGLANDINS
Prostaglandins are a family of compounds comprising 20 carbon aliphatic unsaturated fatty acids.(26) Although first described in 1933, it is only recently that their physiological significance has begun to be appreciated. In relation to articular disease, it is now known that prostaglandin E, (PGE-1) plays a significant role in aiding or promoting the tissue destruction of rheumatoid arthritis.(25,26) Synovial fluid levels of prostaglandins in human rheumatoid arthritis patients are elevated far beyond those in normal joint fluid or joint fluid from patients with osteoarthritis. In vitro studies have shown increased prostaglandin synthesis by rheumatoid synovium and the promotion of bone resorption and articular cartilage destruction by prostaglandins.(27)
To date, data are not available describing prostaglandin levels in synovial fluid from a large number of normal dogs or cats or in those with disease. However, increased amounts of prostaglandins have been found in the joints of dogs injected with known inflammation producing substances, suggesting that, as in humans, synovium of the canine joint produces prostaglandins when inflamed.(10) Prostaglandin levels of synovial fluid have no great diagnostic significance as yet, but they may prove to be valuable in differentiating early immune-mediated synovitis from the synovitis of osteoarthritis.
sjogren
https://www.youtube.com/watch?v=C3e6V0tZIA4
https://www.youtube.com/watch?v=xN6tHrp1LVw&feature=emb_logo
https://www.sciencedirect.com/topics/medicine-and-dentistry/rheumatic-disease
Soft Tissue Calcification
|
heterotopic CALCIFICATION
unorganised deposition of calcium salts. can have dystrophic, idiopathic, and metastatic calcification. |
heterotopic OSSIFICATION
organised deposition of calcium salts |
Dystrophic Calcification
forms in Degenerating, Diseased, Dead tissue (3 d's) despite normal serum and phosphate levels e.g. calcified lymph nodes |
Idiopathic calcification: deposition of calcium in normal tissue despite normal serum and phosphate levels e.g. Sialoliths
Metastatic calcification: minerals precipitate into normal tissue because of higher than normal serum levels of calcium e.g. hyperparathyroidism
Calcified lymph nodes: Classification: Heterotopic calcification - dystrophic. (See Below)
Metastatic calcification: minerals precipitate into normal tissue because of higher than normal serum levels of calcium e.g. hyperparathyroidism
Calcified lymph nodes: Classification: Heterotopic calcification - dystrophic. (See Below)
|
Calcified lymph node (radio)
|
Tonsilar calculi/ tonsilloliths: Classification: heterotropic calcification - dystrophic
|
Tonsilar calculi/ tonsilloliths (radio)
Location: single/multiple radiopacities that overlap the mid portion of the ramus in the region where the dorsal surface of the tongue crosses the ramus in the palatoglossal air spaces
|
Arterial calcification: Classification: heterotopic calcification - dystrophic
arteriosclerosis (Monckerberg's Medial Calcinosis), calcified atherosclerotic plaque
arteriosclerosis (Monckerberg's Medial Calcinosis), calcified atherosclerotic plaque
|
Calcified atherosclerotic plaque
|
Calcified atherosclerotic plaque (radio)
Location: arterial bifurcation, adjacent to the greater cornu of the hyoid bone, C3/C4
|
|
Monckerberg's Medial Calcinosis
Pathogenesis: fragmentation, degeneration and eventual loss of elastic fibres, deposition of calcium within the medial coat of the vessel
|
Mockenberg's Medial calcinosis (radio)
Location: where the carotid or facial A is Periphery: calcific deposits in teh walls outline the artery, appears as radiopaque lines (pipe stem) Internal structure: N/A |
|
Phleboliths: Classification: heterotopic calcification - idiopathic
|
Phleboliths (radio)
Location: in haemangiomas Periphery: round/oval, smooth, up to 6mm diameter Internal: homogeneously radiopaque/laminations/bulls-eye appearance |
|
Triticeous cartilage calcifications
Classification: heterotopic - idiopathic calcification
|
Triticeous cartilage calcifications (radio)
|
|
Rhinolith/Antrolith: Classification: heterotopic - idiopathic calcification
|
Rhinolith/Anrolith (radio)
Location: R - nose, A - antrum (floor of sinus) Periphery: variety Internal: homo or hetero |
Styloid chain ossification: symptomless, Detected by palpation over the tonsil as a hard, pointed suture
Eagle's Syndrome: Clinical: vague - intense pain in pharynx on swallowing, turning head, yawning, Recent Hx of neck trauma, Elongated styloid process and local scar tissue impinge glossopharyngeal nerve
Stylohyoid syndrome: Clinical: vague - intense pain in pharynx on swallowing, turning head, yawning, trismus, temporal headache, vertigo, no recent Hx of neck trauma
Calcified stylohyoid ligament (radio) are thought to be the result of post-tonsillectomy or traumatic scarring. Elongated styloid processes develop from variations in embryological development. Location: mastoid process to ramus and hyoid bone, Shape: joint-like (pseudo articulations),
Internal: homogeneously radiopaque
Internal: homogeneously radiopaque
Calcified Lymph Nodes : How To Treat Them
Calcification is a buildup of calcium in the body tissues. It normally occurs in the bone formations of our body, but can also occur in soft tissues, making them hard. Calcified lymph nodes are frequently seen on x-rays, but are almost always asymptomatic and are generally ignored.
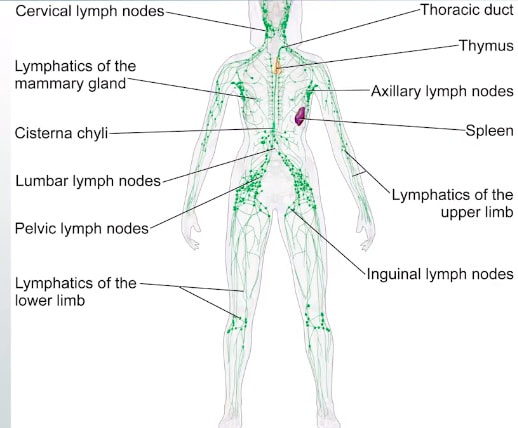
Lymph nodes are a vital component of our immune mechanism: They activate the lymphocytes against bacteria, fungi, and viruses and effectively fight them. The lymph nodes are found in clusters all over our body. They are typically found in the neck, groin and the armpits. The lymph nodes detect infection and make sure it does not spread all over the body. The lymph nodes comprise of lymphatic tissue and are encapsulated.
What Causes Development Of Calcified Lymph Nodes?
Calcification of the lymph node occurs as a consequence to calcium deposits in it during inflammation and swelling. When there is a microbe invading your body, the lymph nodes entrap and screen out anything that triggers infection. Sometimes, after the lymph nodes swell, they may not go back to their original size that they were prior to the infection. The lymph nodes may form a mass from the calcium deposits and this causes calcification of the gland.
Lymph node calcifications most often result from prior granulomatous infections (See below), especially tuberculosis and histoplasmosis which is a disease caused by the fungus Histoplasma capsulatum. Symptoms of this infection vary greatly, but the disease affects primarily the lungs.
Other, less common, causes are sarcoidosis, silicosis, amyloidosis, and calcifications secondary to the treatment of lymphomas (radiation therapy or chemotherapy).
Lymph nodes are a vital component of our immune mechanism: They activate the lymphocytes against bacteria, fungi, and viruses and effectively fight them. The lymph nodes are found in clusters all over our body. They are typically found in the neck, groin and the armpits. The lymph nodes detect infection and make sure it does not spread all over the body. The lymph nodes comprise of lymphatic tissue and are encapsulated.
What Causes Development Of Calcified Lymph Nodes?
Calcification of the lymph node occurs as a consequence to calcium deposits in it during inflammation and swelling. When there is a microbe invading your body, the lymph nodes entrap and screen out anything that triggers infection. Sometimes, after the lymph nodes swell, they may not go back to their original size that they were prior to the infection. The lymph nodes may form a mass from the calcium deposits and this causes calcification of the gland.
Lymph node calcifications most often result from prior granulomatous infections (See below), especially tuberculosis and histoplasmosis which is a disease caused by the fungus Histoplasma capsulatum. Symptoms of this infection vary greatly, but the disease affects primarily the lungs.
Other, less common, causes are sarcoidosis, silicosis, amyloidosis, and calcifications secondary to the treatment of lymphomas (radiation therapy or chemotherapy).
|
Here are some of the likely causes for the development of calcified lymph nodes in your body:
|
|
When a lymph node gets calcified, it is a warning of some other problem in your body. It indicates that there could be either an infection or a tumor mass in the region of the lymph node. Calcification may be due to a scar tissue from an earlier infection or trauma. In cases of some malignancy, the lymph node will be excised for biopsy and to avert the cancer from spreading.
Calcified lymph nodes are like scar tissue from an infection or cancer. The event which caused the calcification of the lymph node may have occurred several years before, additional investigations to ascertain whether the infection is present or not.
Calcified lymph nodes are like scar tissue from an infection or cancer. The event which caused the calcification of the lymph node may have occurred several years before, additional investigations to ascertain whether the infection is present or not.
Classification of granulomatous disorders
Fungi
Histoplasma -
Coccidioides -
Aspergillus -
Cryptococcus -
(Sporothrix, Blastomyces) -
Protozoa
Toxoplasma -
Shistosoma -
Leishmania -
Spirochetes
T. Pallidum -
(T. Carateum, T. Pertenue) -
Mycobacteria
M. Tuberculosis -
M. Leprae -
M. Avian -
BCG vaccine - Bacillus Calmette–Guérin vaccine is a vaccine primarily used against tuberculosis. In countries where tuberculosis or leprosy is common.
M. Kansaii, M Marinum - Mycobacterium kansasii, Mycobacterium marinum
Bacteria
Brucella -
Yersinia -
Vasculitis
Wegeners -
Necrotizing sarcoidal -
Churg-Strauss -
Lymhomatoid -
PAN -
Giant cell arteritis -
SLE -
Immunological aberrations
Sarcoidosis -
Crohn's disease -
PBC -
Peyronies disease -
Histiocytosis X -
Immune complex disease -
Hypersensitivity pneumonitis
Farmer's lung -
Bird fanciers -
Mushroom workers -
Suberosis -
Bagasossis -
Maple bark strippers -
Paprika splitters -
Coffe bean -
Spatlese lung-
Chemicals
Beryllium -
Zirconium -
Silica -
Starch -
Talc -
Neoplasia
Carcinoma-
Reticulosis-
Pinealoma-
Dysgerminoma (Seminoma) -
Reticulum cell sarcoma -
Malignant nasal granuloma -
Other diseases
Whipple -
Cat scratch -
Lymphogranuloma -
Kikuchi -
Buruli ulcer -
Histoplasma -
Coccidioides -
Aspergillus -
Cryptococcus -
(Sporothrix, Blastomyces) -
Protozoa
Toxoplasma -
Shistosoma -
Leishmania -
Spirochetes
T. Pallidum -
(T. Carateum, T. Pertenue) -
Mycobacteria
M. Tuberculosis -
M. Leprae -
M. Avian -
BCG vaccine - Bacillus Calmette–Guérin vaccine is a vaccine primarily used against tuberculosis. In countries where tuberculosis or leprosy is common.
M. Kansaii, M Marinum - Mycobacterium kansasii, Mycobacterium marinum
- Mycobacterium kansasii, which grows well at 37°C and is isolated principally from patients with pulmonary disease
- Mycobacterium marinum is a free-living bacterium, which causes opportunistic infections in humans. M. marinum sometimes causes a rare disease known as aquarium granuloma, which typically affects individuals who work with fish or keep home aquariums
Bacteria
Brucella -
Yersinia -
Vasculitis
Wegeners -
Necrotizing sarcoidal -
Churg-Strauss -
Lymhomatoid -
PAN -
Giant cell arteritis -
SLE -
Immunological aberrations
Sarcoidosis -
Crohn's disease -
PBC -
Peyronies disease -
Histiocytosis X -
Immune complex disease -
Hypersensitivity pneumonitis
Farmer's lung -
Bird fanciers -
Mushroom workers -
Suberosis -
Bagasossis -
Maple bark strippers -
Paprika splitters -
Coffe bean -
Spatlese lung-
Chemicals
Beryllium -
Zirconium -
Silica -
Starch -
Talc -
Neoplasia
Carcinoma-
Reticulosis-
Pinealoma-
Dysgerminoma (Seminoma) -
Reticulum cell sarcoma -
Malignant nasal granuloma -
Other diseases
Whipple -
Cat scratch -
Lymphogranuloma -
Kikuchi -
Buruli ulcer -
