
Madonna of the Pomegranate. Painted in 1487 by Sandro Botticelli
During these years, Art was more about families and less about nations so much that Botticelli painted the pomegranate as the biblical apple.
Pomegranate contains at least 12 different types of estrogens some phytoestrogens and some human identical.
During these years, Art was more about families and less about nations so much that Botticelli painted the pomegranate as the biblical apple.
Pomegranate contains at least 12 different types of estrogens some phytoestrogens and some human identical.
|
Treatment Goals: Manage Pain and Improve Function
Osteoarthritis treatment plans often include exercise, rest and joint care, pain relief, weight control, medicines, surgery, and complementary treatment approaches. Current treatments for osteoarthritis can relieve symptoms such as pain and disability, but there are no treatments that can cure the condition. Although health care professionals can prescribe or recommend treatments to help you manage your arthritis, the real key to living well with the disease is you. Research shows that people with osteoarthritis who take part in their own care report less pain and make fewer doctor visits. They also enjoy a better quality of life. Learn more about treatments for osteoarthritis from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. |
|
Estrogen and Progesterone
Maintaining healthy levels of the reproductive hormones, estrogen and progesterone, can reduce the risk of triggering RA inflammation.
Doing blood tests and addressing these levels of reproductive hormones is a prospective treatment option for patients with RA as joint symptoms are reduced during pregnancy as well as during a woman’s postovulatory stage of the menstrual cycle, when reproductive hormone levels tend to be higher. These types of hormonal changes also put a woman at risk as she ages, when her levels of reproductive hormones naturally decrease. |
Link The Keys to Healthy Female Hormone Function to watch the full video
|
Once she has reached and passed the age of menopause, hormone levels aren’t nearly at the same as they were at an earlier age. It is possible that this lowered hormone level is what causes the onset of this type of arthritis in the joints, and is why this segment of the population experiences this disease more than any others.
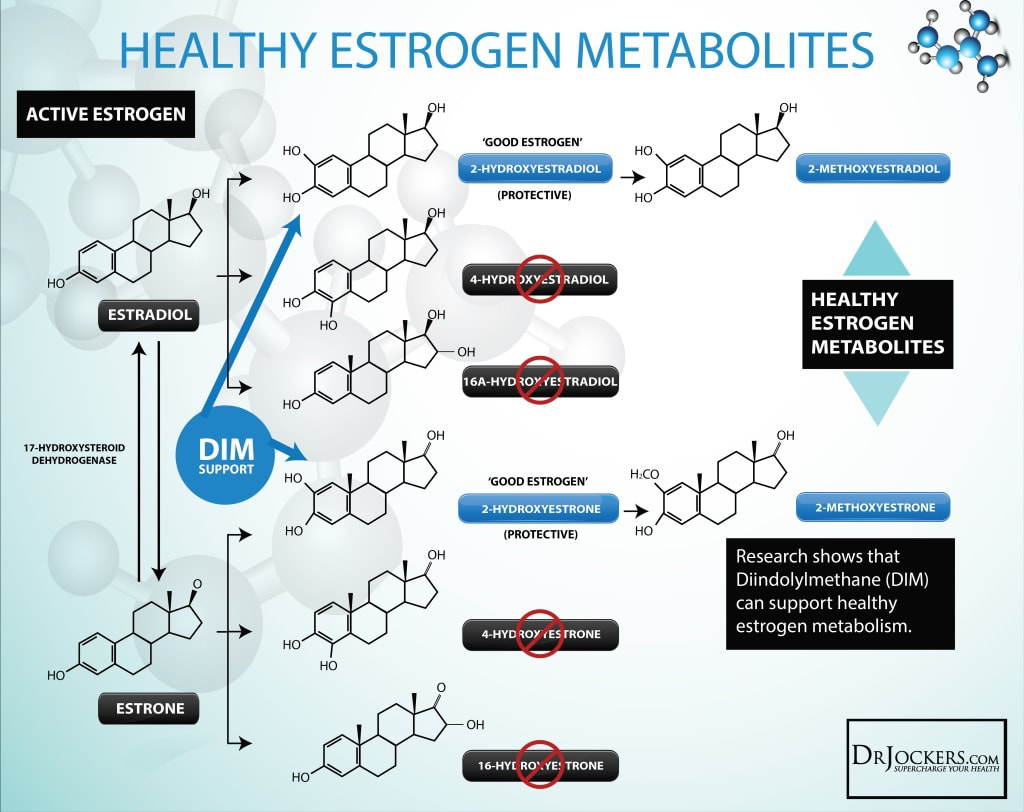
2-Hydroxyestrone, also known as estra-1,3,5-trien-2,3-diol-17-one, is an endogenous, naturally occurring catechol estrogen and a major metabolite of estrone and estradiol. It is formed irreversibly from estrone in the liver and to a lesser extent in other tissues via 2-hydroxylation mediated by cytochrome P450 enzymes, mainly the CYP3A and CYP1A subfamilies.Wikipedia
Osteoclast
Chronic inflammatory arthritis leads to inflammatory bone loss and involves local erosion of articular bone.
This osteo-destructive feature of chronic inflammatory arthritis is a major cause of disability in patients with rheumatoid arthritis.
Osteoclasts are essential for the resorption of mineralized cartilage and subchondral bone in chronic arthritis.
This osteo-destructive feature of chronic inflammatory arthritis is a major cause of disability in patients with rheumatoid arthritis.
Osteoclasts are essential for the resorption of mineralized cartilage and subchondral bone in chronic arthritis.
|
What Is Subchondral Bone?
Subchondral bone is the layer of bone just below the cartilage in a joint. the -chondral refers to cartilage, while the prefix sub means below. Subchondral bone is a shock absorber in weight-bearing joints. |
It has many blood vessels supplying it with nutrients and oxygen and taking away wastes. As cartilage doesn't have its own blood supply, the close association with the vascularized subchondral bone is what keeps the cartilage nourished. These vessels provide over half of the hydration, oxygenation, and glucose for the cartilage.1 The health and function of the subchondral bone will make a difference in the health of the cartilage that lies just above it.
|
|
What hormones increases osteoclast formation
- 1, 25 OH vit D increases: MCSF, RANKL - glucocorticoids: increase RANKL - PTH: increase RANKL How do osteoclasts cause bone resorption - bind to bone via integrin - carbonic and hydrase II produces H+ - H+ is pumped into resorption pit via ATPase pump - lysozymes release enzymes into pit - they are activated by H+ - MCSF and RANKL activate function -calcitionin and INF inhibit function Oestopetrotic model - osteoclasts are not activated or don't function normally - characterized by net accumulation of bone mass - can decrease marrow cavity Pagets Disease Pathogenesis increased vit D receptors -increased RANKL by stroma cells = increase osteoclast number and activity Pagets Ppresentation areas of hyperactive resorption with compensatory increased formation |
Requirements for osteoclast formation - MCSF from osteoblasts -RANKL from stromal cells What inhibits osteoclasts - OPG What hormones decreases osteoclast formation - estradiol - TGF increase OPG Steroid induced osteoporosis pathogenesis inhibits OPG (osteoclast inhibitor) -increases PTH and RANKL -inhibits osteoblast number and activity Consequence of metabolic bone disease in malignancy 1) tumor -> PTHrp 2) tumors -> cytokines = increase number and activity |
2-Hydroxyestrone
|
DIINDOLYLMETHANE
|
|
Phaseolus vulgaris (Fabaceae) - found in fruit, husk, and flower
|
Brassica oleracea var. capitata l. (Brassicaceae) - found in plant and leaf
|
Metabolic disorders result from a malfunction of metabolism. Metabolism is usually working properly. However, in certain situations metabolic disorders occur as a result of not adequate chemical reactions.. The enzymes and hormones are the components responsible for the chemical reactions of metabolism.
Viral Associations: Autoimmune & Estrogen Metabolism. Epstein barr virus (EBV) is associated with autoimmune diseases. ESTROGEN DOMINANCE: VIRUSES & AUTOIMMUNE DISEASE metabolichealing.com/estrogen-dominance-viruses-autoimmune-disease/
Viral Associations: Autoimmune & Estrogen Metabolism. Epstein barr virus (EBV) is associated with autoimmune diseases. ESTROGEN DOMINANCE: VIRUSES & AUTOIMMUNE DISEASE metabolichealing.com/estrogen-dominance-viruses-autoimmune-disease/
The link between rheumatoid arthritis and osteoporosis
Studies have found an increased risk of bone loss and fracture in individuals with rheumatoid arthritis. People with rheumatoid arthritis are at increased risk for osteoporosis for many reasons. To begin with, the glucocorticoid medications often prescribed for the treatment of rheumatoid arthritis can trigger significant bone loss. In addition, pain and loss of joint function caused by the disease can result in inactivity, further increasing osteoporosis risk. Studies also show that bone loss in rheumatoid arthritis may occur as a direct result of the disease. The bone loss is most pronounced in areas immediately surrounding the affected joints. Of concern is the fact that women, a group already at increased risk for osteoporosis, are more likely than men to have rheumatoid arthritis as well.
Examples of glucocorticoid drugs include:
beclomethasone , betamethasone, budesonide, cortisone, dexamethasone, hydrocortisone, methylprednisolone, prednisolone, triamcinolone,
Examples of glucocorticoid drugs include:
beclomethasone , betamethasone, budesonide, cortisone, dexamethasone, hydrocortisone, methylprednisolone, prednisolone, triamcinolone,

|
Nonsteroidal plant estrogens were first identified in the early 1930s, with the discovery that pomegranates,
soybeans, willows, and dates, contain compounds with structural similarity to estrogens. (1) Synthetic glucocorticoids can be more potent than the naturally occurring steroids. They are used to treat many conditions. |
Like rheumatoid arthritis, osteoporosis has no cure. However, medications are available to prevent and treat osteoporosis, including bisphosphonates; calcitonin; estrogen (hormone therapy); estrogen agonists/antagonists (also called selective estrogen receptor modulators or SERMs); parathyroid hormone (PTH) analog; parathyroid hormone-related protein (PTHrp) analog; RANK ligand (RANKL) inhibitor; and tissue-selective estrogen complex (TSEC).
Link The Keys to Healthy Female Hormone Function to watch the full video
|
HormonesCorticosteroids
* A group of hormones that protect the body from infection, exertion, allergic reaction. * Anti-inflammatory! * Can also be given if a patient has: -Insufficient adrenal gland (aka Addison disease)! -Ezema -Asthma -Allergies -Rheumatoid arthritis -Lupus -Crohn's disease Adrenaline A hormone secreted by the adrenal glands, especially in conditions of stress, increasing rates of blood circulation, breathing, and carbohydrate metabolism and preparing muscles for exertion. |
Harvey Cushing (1869-1939)
The person who discovered that people can overdose on corticosteroids. He discovered Cushing's syndrome which is due to over-activity of the adrenal gland due to long time use of corticosteroids. |
|
Cortisol
Everyone has high cortisol from time to time. It’s part of your body’s natural response to threats of harm or danger. But having high cortisol over a longer period of time can have lasting effects on your health including:
|
Adrenaline
|
|
Cortisone
|
Cortisone is the hormone of the adrenal cortex previously known as compound E (17-hydroxy-11-dehydrocorticosterone). ACTH is the pituitary adrenal corticotropic hormone which stimulates responsive adrenal glands to produce cortisone or a cortisone-like steroid such as compound F. (1)
|
Several things can contribute to the development of high cortisol.
Commonly prescribed corticosteroids include:
Steroid medications should never be stopped without gradual tapering. Abruptly stopping can cause low levels of cortisol. This can cause low blood pressure and blood sugar, even coma and death.
Always speak to your doctor before making any changes to your dosing schedule when taking corticosteroids.
EstrogenCirculating estrogen can increase cortisol levels in your blood. This can be caused by estrogen therapy and pregnancy. A high circulating concentration of estrogen is the most common cause of high cortisol levels in women.
.
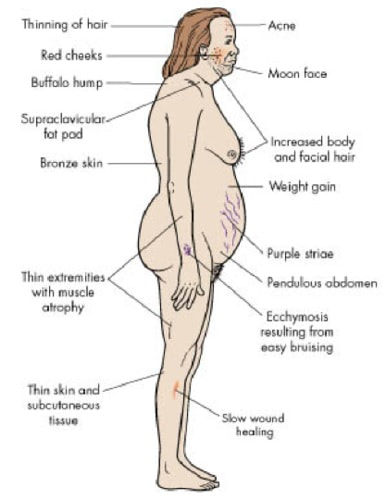
The following result in Cushing's Syndrome (Hypercortisolism) is a hormonal disorder caused by over exposure to the hormone, Cortisol.
To narrow down the underlying cause and help you get your cortisol level back to a safe level.
If you’re experiencing symptoms that may be caused by high cortisol levels, your doctor may recommend the following tests:
- Stress triggers a combination of signals from both hormones and nerves. These signals cause your adrenal glands to release hormones, including adrenaline and cortisol. The result is an increase in heart rate and energy as part of the fight-or-flight response. It’s your body’s way of preparing itself for potentially dangerous or harmful situations. Once the threat passes, your hormones return to their usual levels. This whole process can be a lifesaver. But when you’re under constant stress, this response doesn’t always turn off. Long-term exposure to cortisol and other stress hormones can wreak havoc on almost all of your body’s processes, increasing your risk of many health issues, from heart disease and obesity to anxiety and depression.
- The pituitary gland is a tiny organ at the base of your brain that controls the secretion of various hormones. Issues with the pituitary gland can cause it to under- or over-produce hormones, including adrenocorticotropic hormone. This is the hormone that triggers the adrenal glands to release cortisol.
- Your adrenal glands are located above each kidney. Adrenal gland tumors can be benign (noncancerous) or malignant (cancerous) and range in size. Both types can secrete high levels of hormones, including cortisol. This can lead to Cushing syndrome. In addition, if the tumor is large enough to put pressure on nearby organs, you might notice pain or a feeling of fullness in your abdomen. Adrenal tumors are usually benign and found in approximately 1 in 10 people having an imaging test of the adrenal gland. Adrenal cancers are much more rare.
- Medication side effects
Commonly prescribed corticosteroids include:
- prednisone (Deltasone, Prednicot, Rayos)
- cortisone (Cortone Acetate)
- methylprednisolone (Medrol, MethylPREDNISolone Dose Pack)
- dexamethasone (Dexamethasone Intensol, DexPak, Baycadron)
Steroid medications should never be stopped without gradual tapering. Abruptly stopping can cause low levels of cortisol. This can cause low blood pressure and blood sugar, even coma and death.
Always speak to your doctor before making any changes to your dosing schedule when taking corticosteroids.
EstrogenCirculating estrogen can increase cortisol levels in your blood. This can be caused by estrogen therapy and pregnancy. A high circulating concentration of estrogen is the most common cause of high cortisol levels in women.
.
The following result in Cushing's Syndrome (Hypercortisolism) is a hormonal disorder caused by over exposure to the hormone, Cortisol.
- A tumor of the corticotropes in the pituitary gland
- A tumor in fasicular layer of the adrenal cortex
- Medical treatment with steroids
- Example: The inflammatory activity of the RA significantly correlated with the adrenal cortisol secretion. A 46-year-old woman with rheumatoid arthritis had been on non-steroidal antiinflammatory agents for eighteen years until she developed cushingoid features and hypertension resistant to antihypertensive drugs, due to an adrenal adenoma, in whom rheumatoid arthritis was exacerbated after curing the Cushing's syndrome. (2)
To narrow down the underlying cause and help you get your cortisol level back to a safe level.
If you’re experiencing symptoms that may be caused by high cortisol levels, your doctor may recommend the following tests:
- Cortisol urine and blood tests. These tests measure the levels of cortisol in your blood and urine. The blood test uses a sample of blood drawn from your vein. A test called the 24-hours urinary free cortisol excretion test is used to check your urine. This entails collecting urine over a 24-hour period. Blood and urine samples are then analyzed in a laboratory for cortisol levels.
- Cortisol saliva test. This test is used to check for Cushing syndrome. A sample of saliva collected at night is analyzed to see if your cortisol levels are high. Cortisol levels rise and fall throughout the day and drop significantly at night in people without Cushing syndrome. High cortisol levels at night would indicate you may have Cushing syndrome.
- Imaging tests. CT scans or an MRI may be used to obtain images of your pituitary gland and adrenal glands to check for tumors or other abnormalities.
Osteoporosis, which is characterized by low bone mass and microarchitectural deterioration, is a major risk factor for fractures of the hip, vertebrae, and distal forearm. Hip fracture is the most detrimental fracture, being associated with 20% mortality and 50% permanent loss in function.
https://www.scielosp.org/scielo.php?pid=S0042-96862003000900007&script=sci_arttext&tlng=pt
Hormones
Research has shown that there are a greater number of women who develop RA in their joints, with three times as many patients being female versus male. This leads researchers to believe that female hormones could contribute to the triggering of this disease, making them a risk factor worth considering.
Women who develop RA typically do so somewhere between the ages of 30 and 60 years old. That puts this age range specifically at risk for developing the symptoms associated with RA, the pain and the stiffness in the joints, leading them in search of effective treatment methods in higher numbers than other segments of the population.
Because of this, it appears that maintaining healthy levels of the reproductive hormones, estrogen and progesterone, can reduce the risk of triggering RA inflammation. That makes doing blood tests and addressing these levels a prospective treatment option for patients with RA as joint symptoms are reduced during pregnancy as well as during a woman’s postovulatory stage of the menstrual cycle, when reproductive hormone levels tend to be higher.
These types of hormonal changes also put a woman at risk as she ages, when her levels of reproductive hormones naturally decrease. Once she has reached and passed the age of menopause, hormone levels aren’t nearly at the same as they were at an earlier age. It is possible that this lowered hormone level is what causes the onset of this type of arthritis in the joints, and is why this segment of the population experiences this disease more than any others.
https://www.scielosp.org/scielo.php?pid=S0042-96862003000900007&script=sci_arttext&tlng=pt
Hormones
Research has shown that there are a greater number of women who develop RA in their joints, with three times as many patients being female versus male. This leads researchers to believe that female hormones could contribute to the triggering of this disease, making them a risk factor worth considering.
Women who develop RA typically do so somewhere between the ages of 30 and 60 years old. That puts this age range specifically at risk for developing the symptoms associated with RA, the pain and the stiffness in the joints, leading them in search of effective treatment methods in higher numbers than other segments of the population.
Because of this, it appears that maintaining healthy levels of the reproductive hormones, estrogen and progesterone, can reduce the risk of triggering RA inflammation. That makes doing blood tests and addressing these levels a prospective treatment option for patients with RA as joint symptoms are reduced during pregnancy as well as during a woman’s postovulatory stage of the menstrual cycle, when reproductive hormone levels tend to be higher.
These types of hormonal changes also put a woman at risk as she ages, when her levels of reproductive hormones naturally decrease. Once she has reached and passed the age of menopause, hormone levels aren’t nearly at the same as they were at an earlier age. It is possible that this lowered hormone level is what causes the onset of this type of arthritis in the joints, and is why this segment of the population experiences this disease more than any others.
What is osteoarthritis? Also known as DJD
Degenerative Joint Disease (DJD)
Causes the breakdown of cartilage in joints...leads to pain and stiffness Is NOT inflammatory or systemic like RA rather it is DEGENERATIVE Limits it's attack to individual joints Weight bearing joints are usually affected Most common= hips, knees, spine, MTP joint of big toe, hand PIP/DIP/CMC or thumb Can range from mild to severe |
Physiological changes during OA
Smooth cartilage softens and loses it's elasticity/flexibility
Sections of the cartilage covering the ends of the bones wear away Bones rub together =PAIN Joint loses its normal shape as the ends of the bone hypertrophy... spurs (osteophytes) are often formed where the ligaments and capsule attach to the bone (at the edges) Fluid filled cysts may form Bone and cartilage bits may float in joint space Joint becomes inflamed, stiff, and unstable RESULT= Loss of ROM and PAIN. |
bony hypertrophy
Sed ut perspiciatis unde omnis iste natus error sit voluptatem accusant doloremque laudantium, totam rem.
|
|
Dr Bergman explains how to reverse arthritis. "... your body is designed to heal, it's designed to be healthy, your body can regenerate ... fractured bones heal within 4 to 5 weeks and meniscus can regrow it's alive."
KEY WORDS: carpal tunnel, slip disc, bulging disc, herniated disc, osteoarthritis, MS, fibromyalgia, rheumatoid arthritis, |
|
|
A. Atomic Level Investigation of Biomolecular Interfaces on Bone
https://leelab.berkeley.edu/research.html
A.2. High ionic concentrations of NaCl suppress bone demineralization: Na+ and Cl- ions are the major contributors to the ionic concentration in our bodies. Our recent publication (Kwon et al, JPC 2009) showed that high ionic concentrations of NaCl play a critical role in stabilizing bone crystals. Our findings suggest that typical Na+ and Cl- ion concentrations (140 mM) in extracellular body fluids may play a significant role in bone mineral stability.
A.3. Bone defects accelerate demineralization of bone crystal: Defects in bone minerals play a critical role in the bone remodeling processes. Our recent paper (Kwon et al, Langmuir, 2008) demonstrated that local structural defects on the model bone surfaces significantly accelerated demineralization (Fig. 3A). We characterized demineralization both in the presence and absence of defects. Our characterization showed that defects in bone can be easily removed by exposure to acidic buffer secreted by osteoclasts. Crystal surfaces with defects are dissolved ~100 times faster than non-defected surfaces.
A.3. Bone defects accelerate demineralization of bone crystal: Defects in bone minerals play a critical role in the bone remodeling processes. Our recent paper (Kwon et al, Langmuir, 2008) demonstrated that local structural defects on the model bone surfaces significantly accelerated demineralization (Fig. 3A). We characterized demineralization both in the presence and absence of defects. Our characterization showed that defects in bone can be easily removed by exposure to acidic buffer secreted by osteoclasts. Crystal surfaces with defects are dissolved ~100 times faster than non-defected surfaces.
